Senior Staff Physician Henry Ford Health Detroit, Michigan
Abstract: Statement of the Problem: Odontogenic infections represent a significant and growing source of emergency department (ED) visits, ranging in severity from localized dental abscesses to life-threatening deep space neck infections. Despite their frequency, limited evidence guides which patients require hospital admission versus safe outpatient discharge. Identifying clinical predictors of admission has direct implications for triage decisions, resource utilization, and care quality in the ED setting.
Materials and Methods: We conducted a retrospective cohort study of adult patients (age = 18 years) presenting to emergency departments within the Henry Ford Health System (HFHS) with a primary or secondary diagnosis of odontogenic infection, identified via relevant ICD-10-CM codes (including K04.6, K04.7, K05.20, K05.21, L03.211, and related diagnoses) during Q3 2025. The primary outcome was hospital admission, defined as inpatient admission or placement in observation status, versus discharge. Candidate predictor variables included patient age, sex, presenting vital signs (heart rate, temperature, SpO2), comorbidities (diabetes mellitus, hypertension, chronic kidney disease [CKD], congestive heart failure [CHF], chronic obstructive pulmonary disease [COPD], anemia), and the Charlson Comorbidity Index (CCI).
Methods of Data Analysis: Descriptive statistics were used to characterize the cohort and compare admitted versus discharged patients. Univariable logistic regression was performed for each candidate predictor. Significant univariable predictors (P < .10) were entered into a multivariable logistic regression model. Results are reported as adjusted odds ratios (aOR) with 95% confidence intervals (CI). Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC). All analyses were performed using Python (statsmodels library).
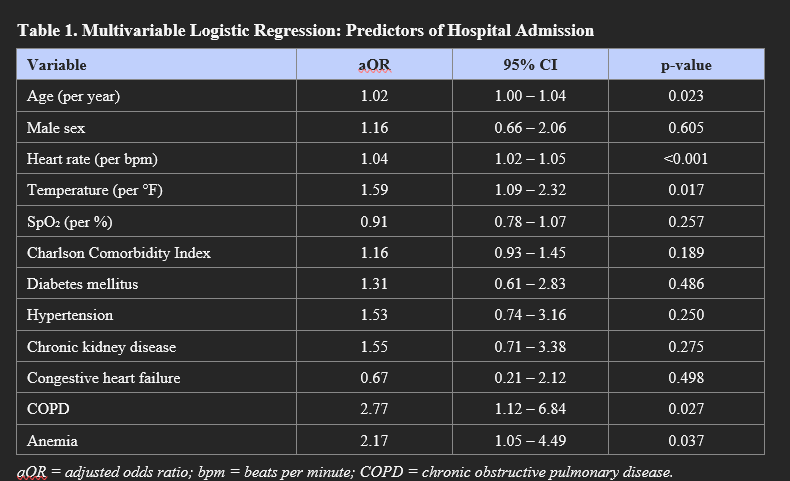
Results: A total of 1,108 ED encounters with complete data were included. The overall hospital admission rate was 5.8% (n = 64). Admitted patients were older (mean age 49.7 vs 36.7 years) and had substantially higher rates of comorbidity compared to discharged patients: diabetes (25% vs 7%), hypertension (48% vs 16%), CKD (25% vs 6%), CHF (12% vs 2%), anemia (31% vs 10%), and COPD (19% vs 3%). Mean Charlson Comorbidity Index was markedly higher in admitted patients (1.08 vs 0.28). On univariable analysis, age, heart rate, temperature, SpO2, CCI, and all comorbidities assessed were significantly associated with admission (all P < .05). On multivariable logistic regression, independent predictors of admission included: older age (aOR 1.02, 95% CI: 1.00 to 1.04, P = .023), elevated heart rate (aOR 1.04, 95% CI: 1.02 to 1.05, P < .001), elevated temperature (aOR 1.59, 95% CI: 1.09 to 2.32, P = .017), COPD (aOR 2.77, 95% CI: 1.12 to 6.84, P = .027), and anemia (aOR 2.17, 95% CI: 1.05 to 4.49, P = .037). Sex, SpO2, CCI, diabetes, hypertension, CKD, and CHF were not independently significant after multivariable adjustment. The model demonstrated good discrimination (AUC = 0.831).
Outcomes Data: The overall admission rate among ED patients presenting with odontogenic infections was 5.8%. Among admitted patients, rates of serious comorbidity were substantially elevated. The multivariable model achieved an AUC of 0.831, indicating strong predictive discrimination. COPD and anemia were the comorbidities most strongly and independently associated with admission after full adjustment.
Conclusions: In this retrospective cohort of ED patients with odontogenic infections, the overall admission rate was 5.8%. After multivariable adjustment, elevated heart rate and temperature, markers of systemic physiologic derangement, along with older age, COPD, and anemia were independent predictors of hospital admission. These findings suggest that vital sign abnormalities and specific comorbidities, rather than diagnosis burden alone, drive admission decisions. These data can inform evidence-based triage and disposition protocols and may support targeted risk stratification tools for emergency physicians and oral and maxillofacial surgeons managing this patient population.
References:
1. Jevon P, et al. Odontogenic infections - a review. Dent Update. 2022;49(1):55-62.
2. Opitz D, et al. Odontogenic infections and their microbiological evaluation. J Craniomaxillofac Surg. 2015;43(9):1843-50.
. Multivariable Logistic Regression: Predictors of Hospital Admission